Pulled Elbow

Moiez gave a 5 min summary on Pulled Elbow:
LOWER LIMB INJURY
THE FOLLOWING IS A SUMMARY OF THIS THURSDAYS TALK ON LOWER LIMB INIJURY
It is surprisingly short considering Orthopoedics is a bottomless pitt of detail . This brief runthrough injury to the lower limb highlights the big issues from ourside of story . It is not important to know the difference between the treatment of an intracapsular Neck of Femur fracture and an intertrochanteric fracture .It is however crucial to understand that delay to operation of either ( past 48 hours ) impacts heavily on mortality and how to avoid this by making sure all the anaesthetic “tick box’s” are ticked. It is also important to make sure the patient is not in pain (hence the emphasis on regional anaesthesia
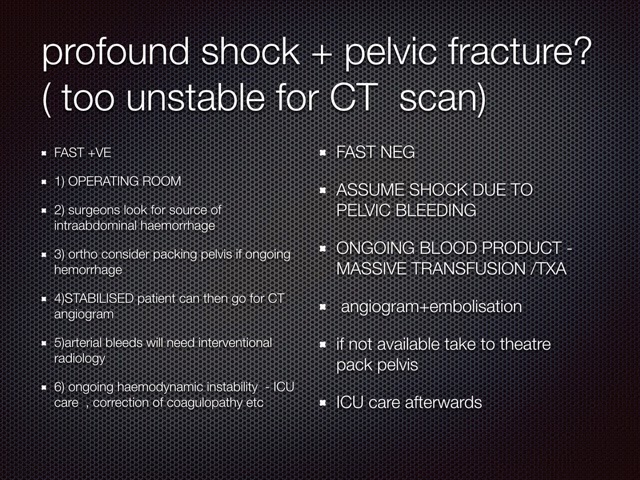
PELVIC FRACTURE IS THE FIRST
here is a link to a great EMRAP TALK ( 2014) on contemporary approach to exanginating pelvic trauma
https://d140vvwqovffrf.cloudfront.net/media/segment/original/972c3fcf990eca3d477367e6d9b572897e0e1aa9.mp3
(if the link above doesnt work just select it and past into your browser )
scot wingart ( http://emcrit.org/podcasts/severe-pelvic-trauma/ ) gives a good up to date summary on the emergency managment of pelvic injury and covers most of the topics in the talk
In the patient who is stable enought to go to CT , usually the CT angiogram will reveal the need for either embolisation via the angiosuite or OR for solid organ injury or ruptured hollow viscous .
low pressure venous bleeding often stabilises by good intensive care but may need packing
In the patient who is unstable ( ie BP <<100) these patients are devided into those who likely have intraabdominal injury as a cause ( ie FAST POSITIVE ) and those that dont
the next important orthopoedic injury is the hip fracture ( obviously less likely high speed trauma and more likely old person
CRITICAL POINTS FOR ED
These guys need their operation in 48 hours less ( or else they do worse ) and they also need pain relief
to faciliate their speed to OR we need to make sure all the pre op boxes are checked and hence the need for a NOF pathway
the following slide shows you what is important to anaesthetic doctors taking a patient to theatre
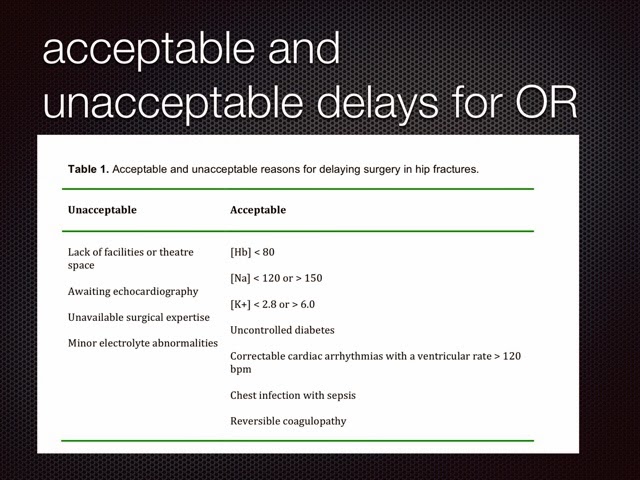








so make sure these tests are done
the next most important thing is to perform a femoral nerve block
if you havent a lot of exeperience use lignocaine 1% and use about 20-30 mls ( avoid LATS)
and look at this link for an indepth demonstration on how to do a fascia iliaca block
http://3lliottjody.wistia.com/medias/0g25pucqw5 ( copy and paste this into your browser )
moving down the leg : femoral shaft fractures can loose buckets of blood so you should predict and correct this . A Thomas splint ( or equivalent ) is necessary for pain relief and to stop bleeding. Make sure you give a femoral nerve block
knee fractures are the domain of the orthopoeidic service . Our job is not to miss any injury that might need earlier follow up or suggest sigficicant ligamentous or even vascular injury
the following xrays are ones that we should all be able to diagnose and get prompt orthopeodic consultation on
1) knee dislocation should be suspected on history and any significant intraarticular fracture . Have a low threshold for getting an angiogram ( to avoid amputation and litigation ) . ANKLE /BRACHIAL ABIs > 90 % have a good negative predictive value and maybe a useful adjunct
2) the segond fracture suggests a medial injury : collateral ligament / AC and meniscal injury (the unhappy triad )
3) the reverse segond suggests similar pathology on the medial side
4) tibial plateau fractures can be subtle
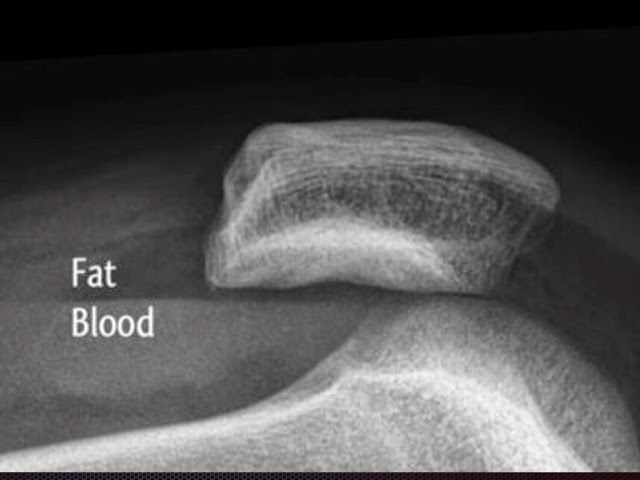
5) the FBI sign is give away for significant fracture ( fat blood interface )
6) dont foreget the massoneuvre fracture
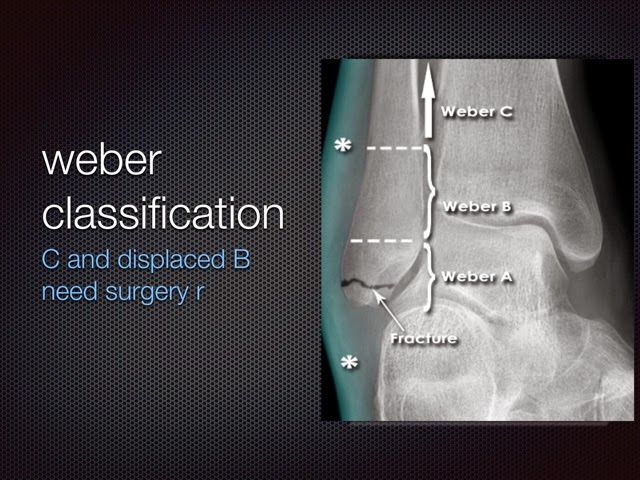
7) ankle fractures are common in ED . Its important to know that a weber B or C are the ones that need surgery
8) bimaleolar and trimaleolar fractures need reduction in ED
9) consider a sciatic / POP fossa block if you cant adminster procedural sedation follow this link for the how to video , remember that it takes half an hour to work
( copy and paste this link http://3lliottjody.wistia.com/medias/vkw4qsewbx )
1) the ankle is best put back in dorsiflexion / traction and pressure backward along the direction of dislocation
11) this is a lisfranc fracture and often needs surgery ( subtle lisfrancs can be missed ) the whole point of the the oblique food xrays to is expsoe the alignement of the lisfranc articulation
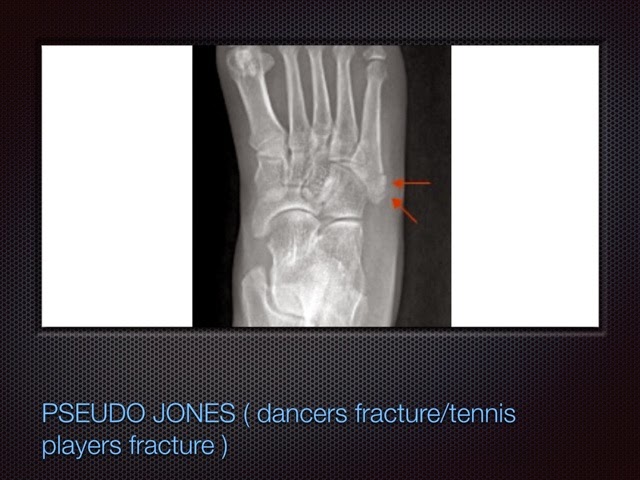
12) Jones fracture bad . Psuedo Jones good . growth plate lines run parallel to axis of bone and would be embarrasing to mistake as a fracture


