 |
|||
| 16 Jul | Induction | ||
| 23 Jul
UPPER AIRWAY |
Dr Babikir : Topic review – Acute upper airway obstruction
5 min topic: oculogyric crisis (Olupitan) |
Dr Lee : Practical Session – Airway manouvres | Dr Sweeney : Audit Cycle
Podcast
|
| 30 Jul | Dr Zahalka: Topic review – Acute anaphylaxis
5 min topic: pulled elbow (Eltahir) |
Dr L Cunningham : Simulation – Acute airway emergencies | Dr Harris
X-ray of the Week |
| 6 Aug | Dr Broderick: Topic review – Croup + Stridor in Children
5 min topic: ring removal (Babikir) |
Dr Hussain : Journal Club/Debate – Video-assisted laryngoscopy | Mr Hickey
ECG of the Week |
| 13 Aug | Dr Flynn/ Dr L Cunningham: Morbidity +Mortality 13 Jul-12 Aug | ||
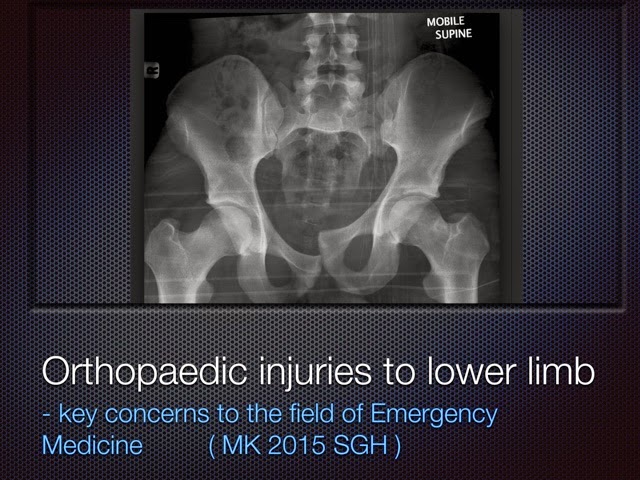
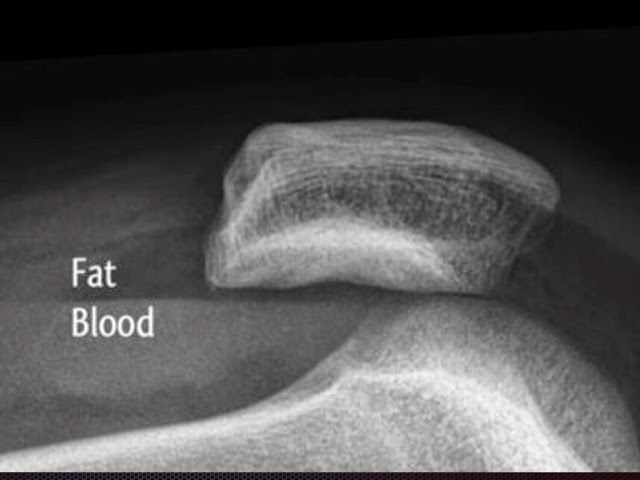
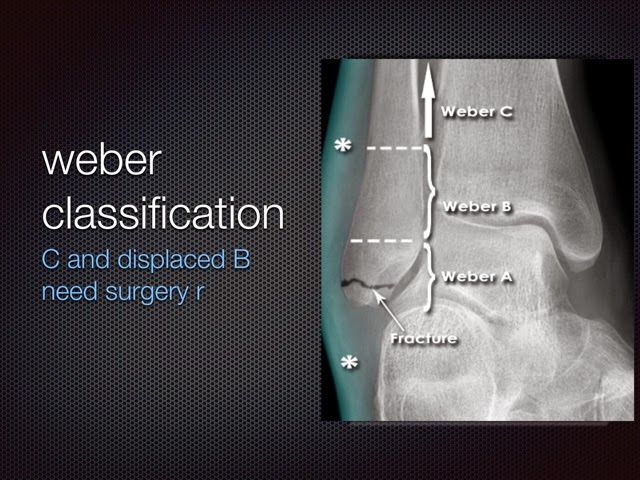
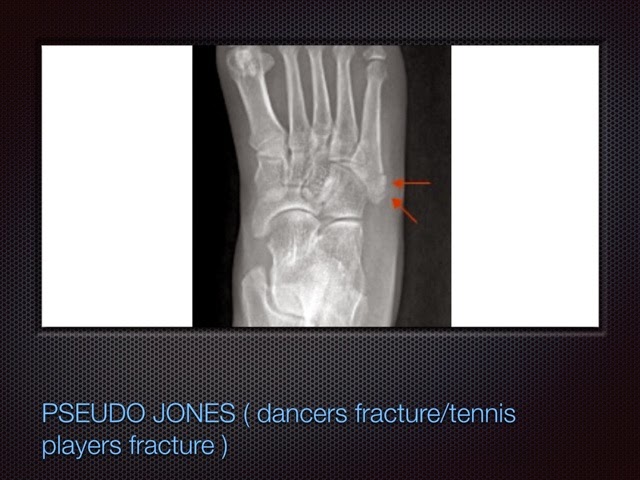
THE FOLLOWING IS A SUMMARY OF THIS THURSDAYS TALK ON LOWER LIMB INIJURY
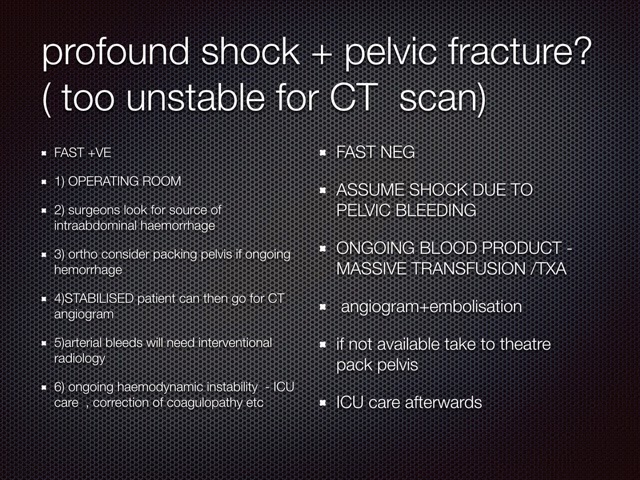
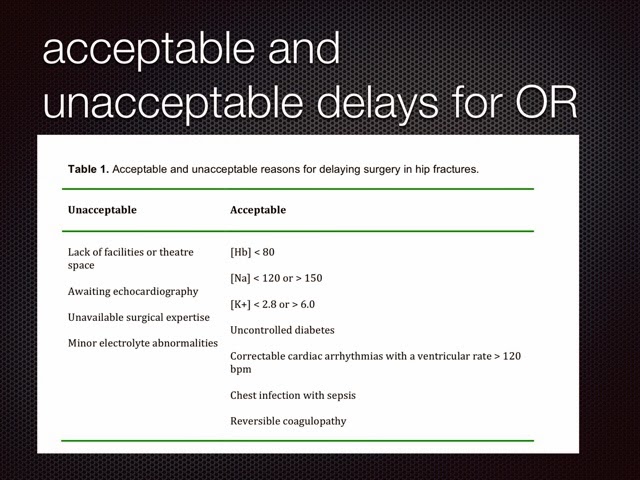








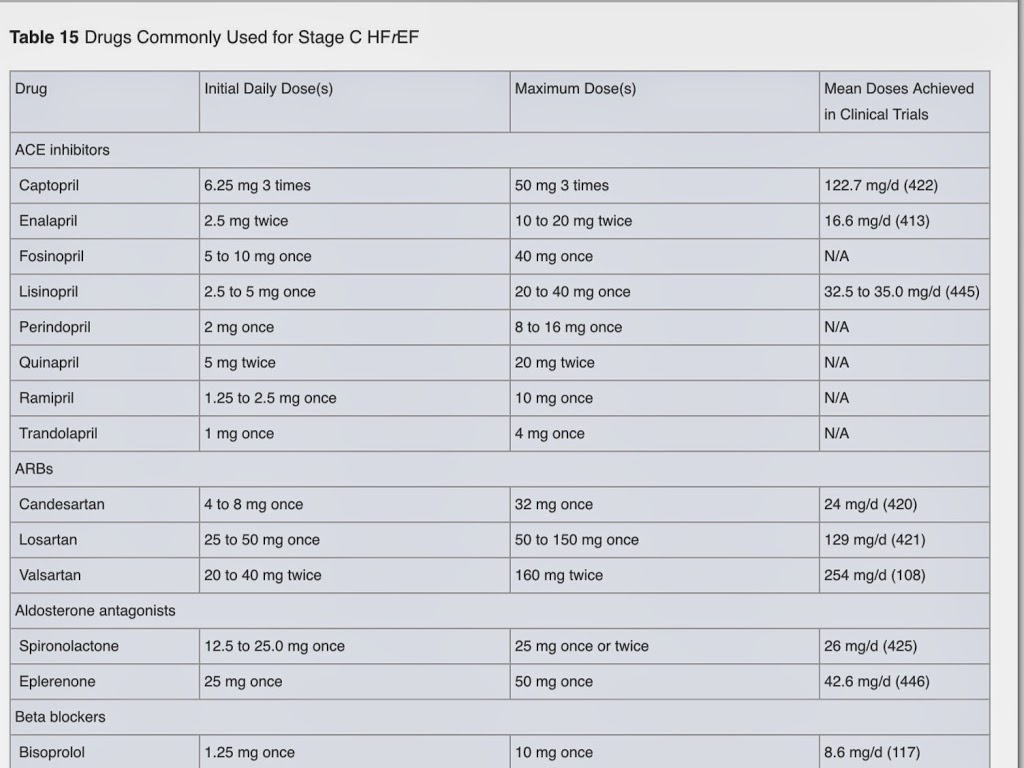
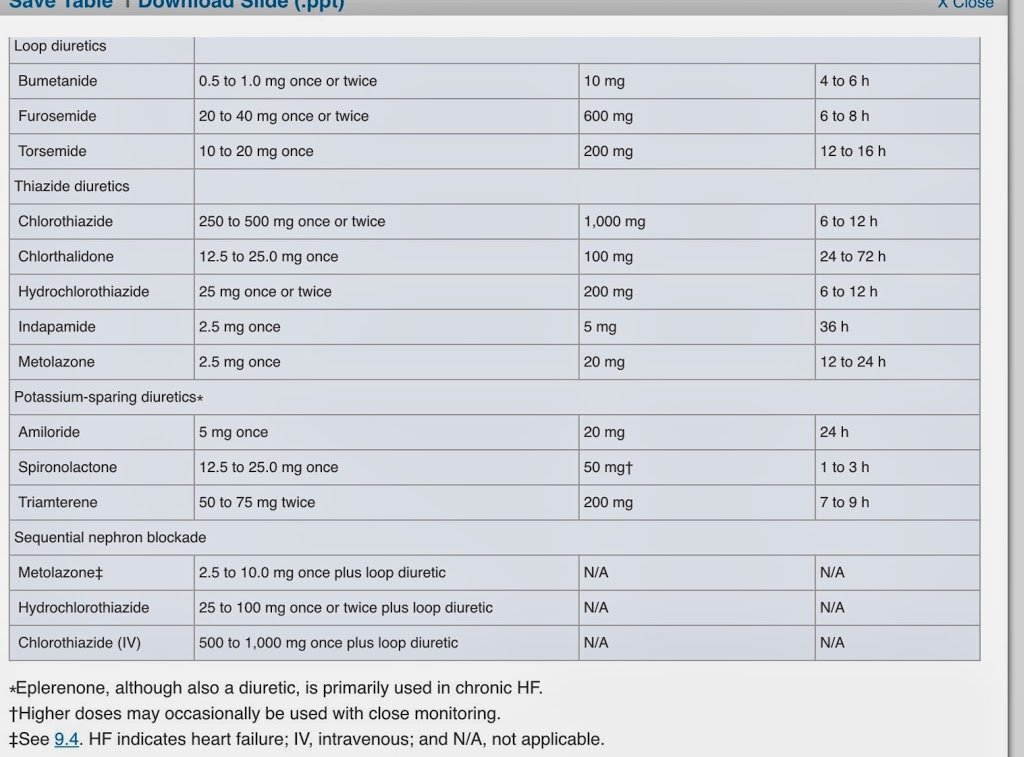
Persistent uncontrolled nyhc grades 2-4 :
WELCOME TO SLIGO ED TEACHING BLOG (EMSLIGO.BLOGSPOT.IE) NOV / DEC 2014
The purpose of this blog is to store teaching talks and other information
The idea is that each talk has a 1 page summary. posted here and links to references/websites used
The links on this page are a great start to finding information for your talks
There will be a (very flexible ) five week cycle
Week1 : NCHD / medical student talks – 4 10 minute talks ( strickly 10 mintues as we have short attention span ) .summary posted here(email me your summary with links mickilleen@gmail.com)
Week 2 : NCHD / medical studtent talks
Week 3 : simulaiton training
Week 4: NCHD / medstudent talks
Week 5: M/M ( review of interesting patients in Resus – keep a patient sticker so you can look up what happened to your patient and present it ) A middlegrade doc or consultant will oversee this .
There will be an OSCE type quiz on topics from these talks ( we will ask each presenter to create an OSCE type question ) this will happen once a term ( so pay attention to the blogsite !)
TOPICS WILL INCLUDE : (red denotes what we have partially covered so far )
1) Management of Acute cardiac emergencies including ACLS review
2) Management of acute respiratory emergencies including Airway management and RSI )
3) Management of acute Neurological Emergencies including CVA (SAH/thrombolysis debate / stroke and TIA guidelines / syncope )
4) Vascular Catastrophes . AAA/ dissection / cardiac Tamponade
5) Trauma management – Recent updates eg ICEM , Damage control resuscitation / crash 2 trial / TTM trial
6) Orthopaedic injuries ( pelvis / longbone / hand and foot / soft tissue injuries to shoulder , knee , wrist and ankle
7) The focussed clinical exam in 2014 – Different Joints / formal Cardiac exam / neurological examination .
8) ULTRASOUND TRAINING – (THREE LECTURES , LOGGING SCANS , SUPERVISION AND TESTING )
9) Paediatric Emergencies ( Assessment of the unwell child / PALS / APLS / APLS review / NAI
10)Interpretation and management of Acute Electrolyte disturbances (hyperkaleamia / acid base / hyponatremia / Hypernatremia / DKA / Honk / Acute renal failure )
11) The critically ill patient – Sepsis bundles / BOIC / Post cardiac arrest management / post intubation check list / inotropes / antibiotics in serious sepsis
12) Toxicology – general approach / Specific and common life-threatening overdoses. Seratonin and anticoholinergic syndrome
THIS MONTHS TOPICS
WEEK ONE ( 13th Nov) – SUMMARY OF ESSENTIALS OF EM CONFERANCE (no NCHD TALKS)
WEEK TWO ( 20 November ) 4 talks in total :
Moving on to medical emergencies , this weeks teaching is brought to you by the elelement Na !


This week we have the following / talks discussions
4) Ultrasound guided nerve blocks in the ankle and the femoral nerve block

Important references here
5) Damage control resuscitation ( if Safras is back from overseas)