Teaching 31 st August 2014 SGH DEM
1) post lumbar puncture headache – Muhammad case presentation and discussion
2) introduction to ultrasound use in the emergency department – mick killeen
3) FOAM , emergency medicine resources online
Please pick a website that you use ( or will use from now on ) and present a five minute talk based around some clinical question and how and why you use this particular source. Below are 2 examples
Clinical question
Background : everywhere I work people seem to have strong opinions about thrombolysis in stroke and the world seems to be devided on their interpretation of the literature – where can I get a good pro and con review on this subject ?
Clinical question
What are the controversies around thrombolysis in acute ischemic stroke
Chosen website ( 3 chosen)
Emcrit – why ? Because I have followed his blogs for years and have grown to trust his blogs and podcast. They are well referenced , make scientific sense and are cutting edge http://emcrit.org/podcasts/tpa-for-ischemic-stroke-debate/
David Newman – a well known cynic and very knowledgeable ed physician who published on a well known website known as the NNT
Plus EMA ONLINE ( emergency medical journal of Australia ) – why ? because I get it free through college of em and I remember seeing this article which was a ballanced counter argument in favour of thrombolysis.
http://onlinelibrary.wiley.com/enhanced/doi/10.1111/1742-6723.12046/
Example 2 .
Clinical question : does tamsulosin help patients in ed with renal colic?
Chosen website : http://thesgem.com/2014/04/sgem71-like-a-rolling-kidney-stone-a-systematic-review-of-renal-colic/
Why : well actually looking for bestbets and cochrane articles but found this one first and it made a lot of sense I then also looked at this site and saw a debate raging in the replys. It answered my question for me ( for now)
http://www.emlitofnote.com/2014/04/sadly-inadequate-cochrane-review-of.html
If you are not sure of a topic check with a senior.
Thanks in anticipation
Mick
( The cycle to work last week)













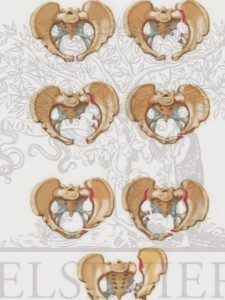 EXANGUINATING PELVIC TRAUMA – MICK and Safa link to MICKS PELVIC FRACTURE TALK HERE
EXANGUINATING PELVIC TRAUMA – MICK and Safa link to MICKS PELVIC FRACTURE TALK HERE 











{kind=link}