 Article published in the Sligo Champion re the Art in the ED Waiting Room collaboration with Sligo Grammar School students
Article published in the Sligo Champion re the Art in the ED Waiting Room collaboration with Sligo Grammar School students
ICEMT Guide to Training in Emergency Medicine in Ireland
The Irish Committee for Emergency Medicine Training (ICEMT) has recently updated its Guide to Emergency Medicine Training in Ireland.
Anybody interested in pursuing a career in EM in Ireland should read.
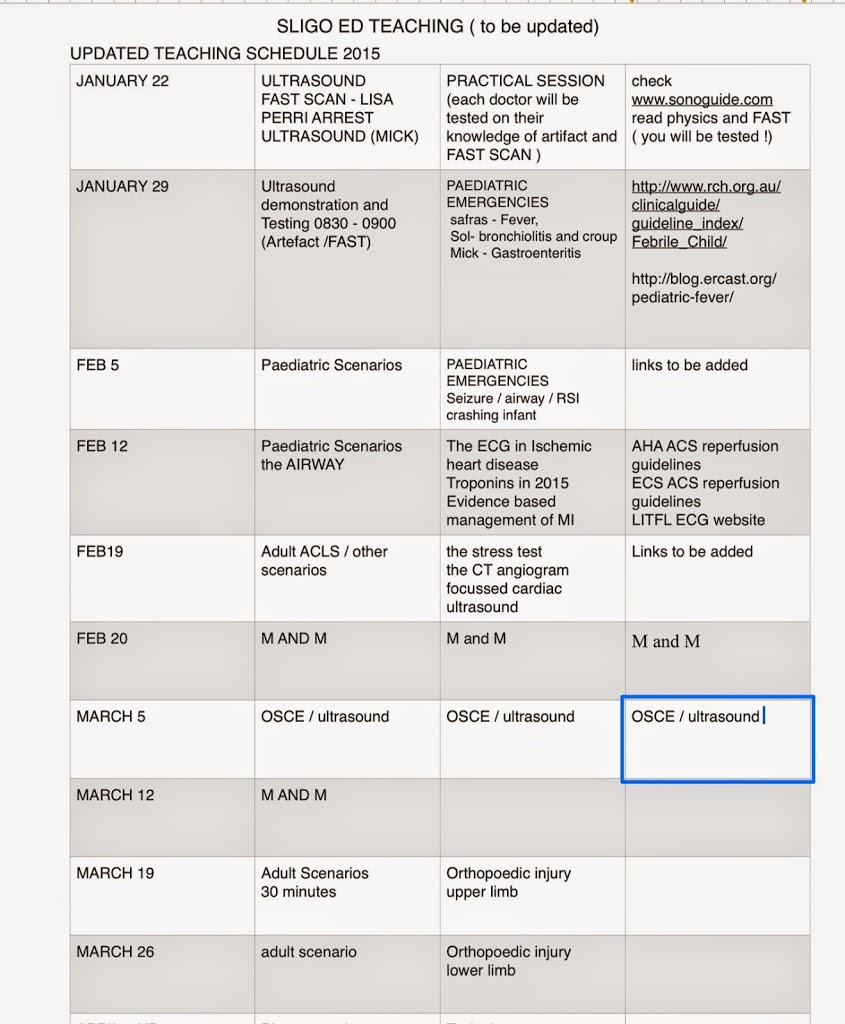
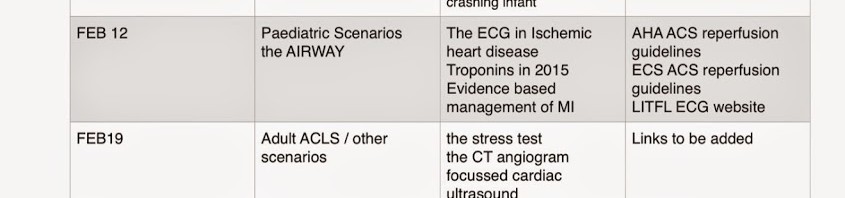
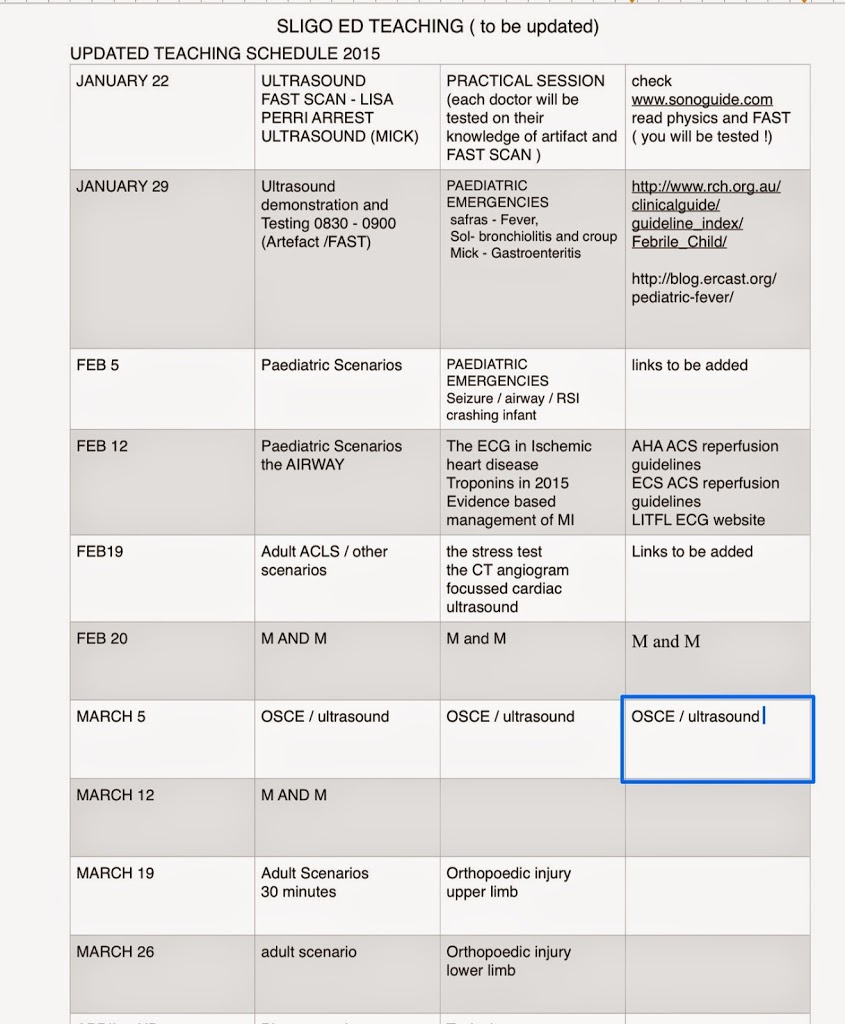
ED Teaching Schedule 2015
Opinion piece on Emergency Medicine in Ireland published in The Irish Times
Fergal Hickey’s piece regarding the future of Emergency Medicine in Ireland published in today’s Irish Times
ED teaching for the beginning of the new year
FCEM Success for Karen
Congratulations to Dr Karen Harris, our current SpR, who passed her final FCEM exams today.
All ED staff delighted
Summary of heart failure talks
summary heart failure talks
thanks to Safras and Mohamed for the talks on heart failure
Below is a summary of take home points
1) new guidelines are out on Heart failure ( nice guidelines ) as of OCTOBER 2014- click on image above for link to FREEDOWNLOAD
. These guidelines are 100s of pages long and reflect the opinion of 100s of clinicians , researchers and patients
. These guidelines are 100s of pages long and reflect the opinion of 100s of clinicians , researchers and patients
There is a de-emphasis on NIV and GTN which doesnt reflect our real world. This is not the fault of the guidelines because neither treatments have much effect on long term survival . I dont believe we can prove their efficacy in terms of short term survival because it would be unethical to do RCTs that involve withholding these treatments on patients in distress in ED
The take home points ( their best interpretation of evidence and expert advice )
Heart failure is the the commonest cause for hospital admissions to hosptial in the over sixty fives
Acute Pulmonary Oedema – is the commonest True ED emergency related to heart failure . The blood pressure is preserved or even high ( I find the pathophysiology behind this hard to fully understand as the usual causes such as mi or Ischemia are not culprits . It is said that there is often a diastolic component , so these patients often have the risk factors for diastolic dysfunction such as diabetes and hypertension )
Assessment
1) acutely the main things are a preserved or high blood pressure and wet lungs ( creps) . When this clinical finding is not obvious ( eg in an obese patient with a history of COPD or risk factors for PE ) , bedside ultrasound has a new and crucial role
Treatment
2) traditional approach is oxygen , frusemide , morphine , nitrates and consider NIV
3) a more rational priority ( and reflective of current ED Practice ) is
Oxygen – best given via NIV ( whatever you have BIPAP or cpap )
Frusemide – standard iv dose ( doesn’t really matter what that is but usually the patients oral dose is given iv)
Gtn ( given first under the tongue 2 sprays = 400mcg) and then as an infusion starting high and lowering if patient becomes hypOtensive eg start at 100mcg per minute or even more ( double this )
congestive heart failure with preserved blood pressure
Assessment.
The crucial points about diagnosis are BNP and a good clinical exam with good basic tests ( ecg/cxr/labs) . The patient should then get an echo (best as in patient ) and this should be a formal one as valvular heart disease needs to be ruled out and this is not yet in the domain of a basic ed bedside echo. Of course it would not be unreasonable to assess EF on bedside echo eg by eye ball estimation or EPSS
Important Inpatient recommendations and guidelines
1) The need for heart failure patients to be linked in to Specialist Clinics
This is an evidence based recommendation and may be because all the things that comes with specialist clinics eg attention to detail / community outreach etc and addressing risk factors :
– dietary and life style measures
– blood pressure / cholesterol / weight / obviously smoking sessation
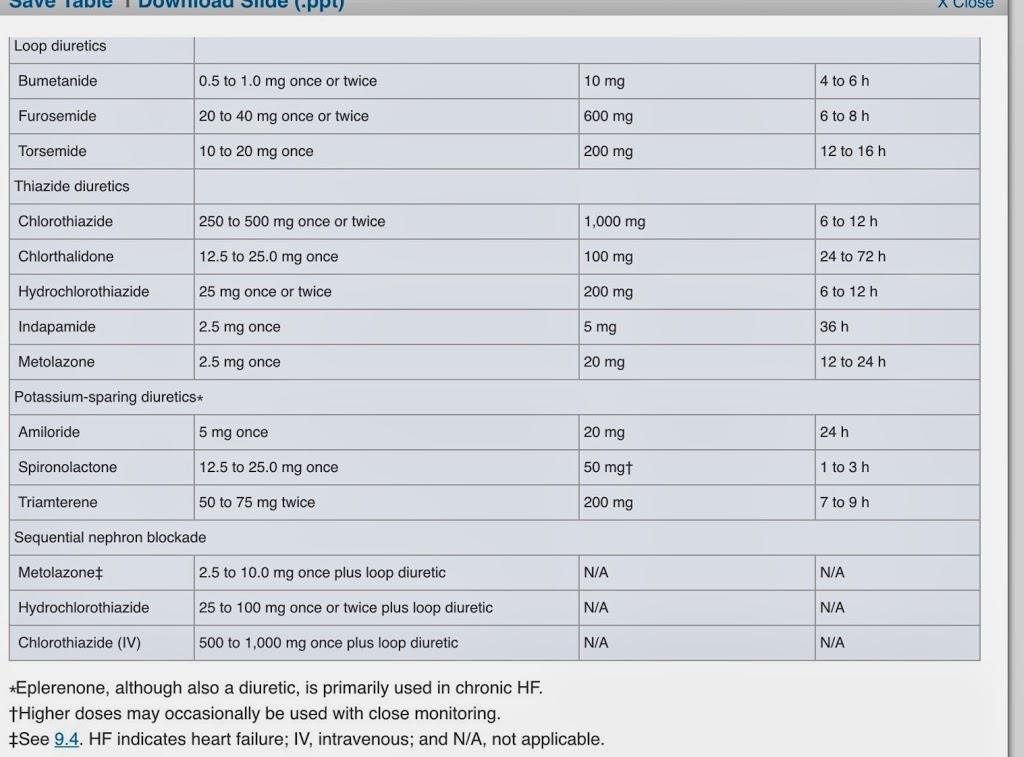
medication
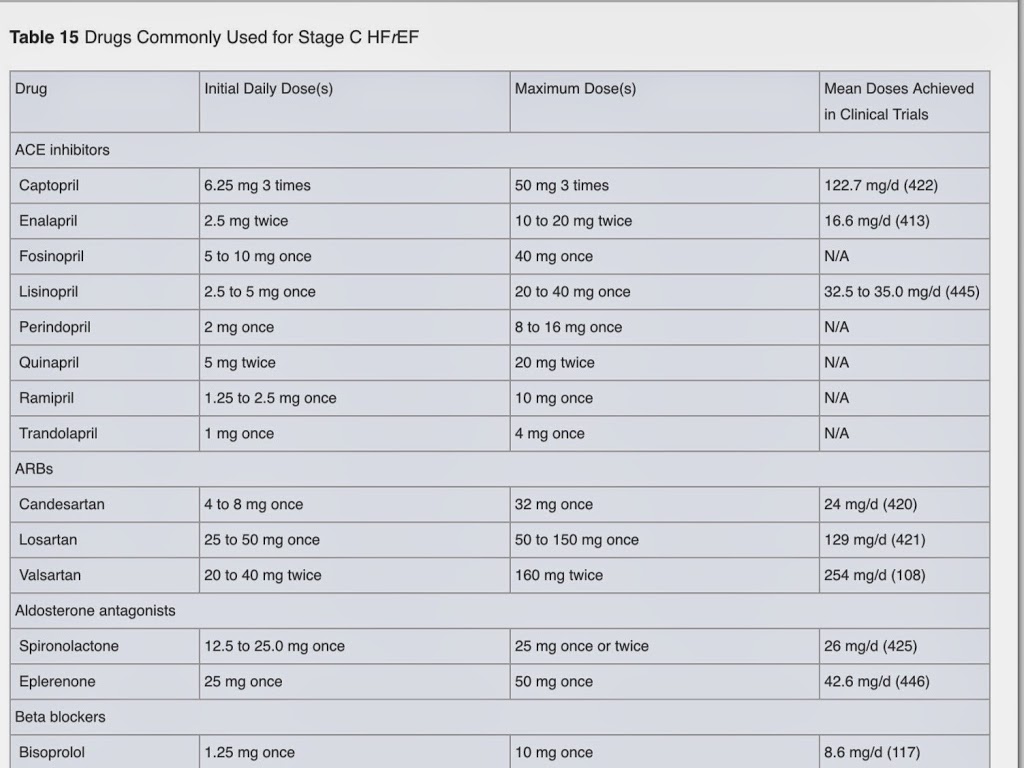
See table attached below of appendix in guidlienes about drug doses
take home points
– give an ace inhibitor ( or equivalent … if possible ) -eg start enalapril 2.5 mg daily and get GP to oversee increments up to ……..
– add a betablocker if patient is stable .that means out of ED , off iv diuretics etc . cardivolol / metoproplol succinate / bispoprolol being evidence based . Better to add a betablocker than increase dose of ace inhibitor according to the guidelines . eg bisoprolol 1.25 mg daily increasing over weeks to
– if giving a betablocker add a thiazide as ankle swellling is a problem
Persistent uncontrolled nyhc grades 2-4 :
– add in spironolactone ( or equiv anti aldosterone equivalent ) —eg
– add in digoxin —
FINALLY
tNOT INCLUDED IN THE NICE GUIDELINES THE COOL STUFF
1) ULTRASOUND
Bedside ultrasound really has such a useful and now evidence based role to play in acute assessment not the least of which includes
IVC assessment when fluid loading
left heart gestalt EF estimation and EPSS
lung assessment – lung rockets or B lines and response to therapy
rule out right heart strain
2)
The high end stuff -REBOA / AORTIC BALLOON COUNTER PULSATION
when are these things to be considered
NOVEMBER DECEMBER TEACHING BLOG FOR SLIGO ED
WELCOME TO SLIGO ED TEACHING BLOG (EMSLIGO.BLOGSPOT.IE) NOV / DEC 2014
The purpose of this blog is to store teaching talks and other information
The idea is that each talk has a 1 page summary. posted here and links to references/websites used
The links on this page are a great start to finding information for your talks
There will be a (very flexible ) five week cycle
Week1 : NCHD / medical student talks – 4 10 minute talks ( strickly 10 mintues as we have short attention span ) .summary posted here(email me your summary with links mickilleen@gmail.com)
Week 2 : NCHD / medical studtent talks
Week 3 : simulaiton training
Week 4: NCHD / medstudent talks
Week 5: M/M ( review of interesting patients in Resus – keep a patient sticker so you can look up what happened to your patient and present it ) A middlegrade doc or consultant will oversee this .
There will be an OSCE type quiz on topics from these talks ( we will ask each presenter to create an OSCE type question ) this will happen once a term ( so pay attention to the blogsite !)
TOPICS WILL INCLUDE : (red denotes what we have partially covered so far )
1) Management of Acute cardiac emergencies including ACLS review
2) Management of acute respiratory emergencies including Airway management and RSI )
3) Management of acute Neurological Emergencies including CVA (SAH/thrombolysis debate / stroke and TIA guidelines / syncope )
4) Vascular Catastrophes . AAA/ dissection / cardiac Tamponade
5) Trauma management – Recent updates eg ICEM , Damage control resuscitation / crash 2 trial / TTM trial
6) Orthopaedic injuries ( pelvis / longbone / hand and foot / soft tissue injuries to shoulder , knee , wrist and ankle
7) The focussed clinical exam in 2014 – Different Joints / formal Cardiac exam / neurological examination .
8) ULTRASOUND TRAINING – (THREE LECTURES , LOGGING SCANS , SUPERVISION AND TESTING )
9) Paediatric Emergencies ( Assessment of the unwell child / PALS / APLS / APLS review / NAI
10)Interpretation and management of Acute Electrolyte disturbances (hyperkaleamia / acid base / hyponatremia / Hypernatremia / DKA / Honk / Acute renal failure )
11) The critically ill patient – Sepsis bundles / BOIC / Post cardiac arrest management / post intubation check list / inotropes / antibiotics in serious sepsis
12) Toxicology – general approach / Specific and common life-threatening overdoses. Seratonin and anticoholinergic syndrome
THIS MONTHS TOPICS
WEEK ONE ( 13th Nov) – SUMMARY OF ESSENTIALS OF EM CONFERANCE (no NCHD TALKS)
WEEK TWO ( 20 November ) 4 talks in total :
evidence based management of heart failure acutely and as an outpatient
use up to date recognised guidelines ( ie 2012+ ) – UK / canadian / ESC / AHA and FOAM
for talks 1 and 2 suggest you base it around 3 cases
talk 1 ) – emergency dept ASSESSMENT of flash pulmonary Oedema / cardiogenic shock / undifferentiated decompensated heart failure
talk 2 ) – emergency department MANAGEMENT of flash pulmonary Oedema / cardiogenic shock / undifferentiated decompensated heart failure ( including heroic things like REBOA or IABC )
talk 3) – outpatient MANAGEMENT and investigations of heart failure – drugs / lifestyle modification/ supportive care / prognosis
talk 4 ) lung ultrasound in an emergency medicine setting focus on A and B lines etc – Registrar
—————————————————————————————————————–
Week THREE
—————————————————————————————————————–
Week THREE
1) DDimer in pregnancy and the over 50s – new guidelines -http://rebelem.com/age-adjusted-d-dimer-testing/ and http://www.perinatology.com/Reference/Reference%20Ranges/D-Dimer.htm
2+3)2 talks aortic dissection – assessment and management in the emergency department ( two talks ) assessment = hx/exam/INVx mangement= resus/defintive tx/ consultation / disposition and other issues (controversies and pit falls , prognosis )
4+5) 2 people : treatment of DVTs of the lower limb , below and above knee – the options and controversies for a start check : http://stemlynsblog.org/new-nice-guidance-on-investigation-of-dvt-in-the-ed/
debate for and against below knee dvt anticoagulation
week 4
Simulation training
week 5
M/and M
Simulation training
week 5
M/and M
Sligo Emergency Department shortlisted for two 2014 Healthcare Innovation Awards
Sligo ED has been shortlisted in two categories for the 2014 Healthcare Innovation Awards.
Innovation – Clinical Area : A safe protocol for paediatric procedural sedation in the ED
Patient Experience: ART in the waiting room
Congrats to all staff involved
http://www.healthawards.ie/2014-shortlist/