Consultant post advertised. For details see link:
http://www.publicjobs.ie/publicjobs/campaignAdvert/23140.htm
Consultant post advertised. For details see link:
http://www.publicjobs.ie/publicjobs/campaignAdvert/23140.htm
Unfortunately, Dr Mick Killeen is returning to New Zealand after a year at the ED in Sligo.
We had a great year with him on our team, and he’ll be sorely missed

 In order to bid him farewell , the ED crew (that weren’t on duty) spent the afternoon on Lough Gill learning to Stand Up Paddle (SUP) with SUPForAll. In treacherous conditions, the ED staff braved the elements.
In order to bid him farewell , the ED crew (that weren’t on duty) spent the afternoon on Lough Gill learning to Stand Up Paddle (SUP) with SUPForAll. In treacherous conditions, the ED staff braved the elements. 
Celebratory meal, and awards ceremony that evening.
For more photos see www.facebook.com/SUPforall





Middle Grade Post Available July 2015
 There is an opportunity in July 2015 for a Middle Grade in Emergency Medicine. Our trainees have a good past record of getting places on Advanced Specialist Training Schemes in Emergency Medicine in Ireland, UK, and Australasia. The rota is European Working Time compliant with very few night shifts, and one-in-four weekends.
There is an opportunity in July 2015 for a Middle Grade in Emergency Medicine. Our trainees have a good past record of getting places on Advanced Specialist Training Schemes in Emergency Medicine in Ireland, UK, and Australasia. The rota is European Working Time compliant with very few night shifts, and one-in-four weekends.
Candidates are expected to have a keen interest in gaining experience in Emergency Medicine at a Middle Grade level, with previous EM experience essential.
For further details on the post and how to apply contact ed.admin@hse.ie, or ramona.coen@hse.ie
Other Registrar Posts Available in other specialties at Sligo Regional Hospital for July 2015
There are also opportunities at Registrar Level at Sligo Regional Hospital in the following specialties:
For further details on these posts and how to apply contact ramona.coen@hse.ie
Middle Grade Post Available July 2015
There is an opportunity in July 2015 for a Middle Grade in Emergency Medicine. Our trainees have a good past record of getting places on the National Advanced Specialist Training Scheme in Emergency Medicine. The rota is European Working Time compliant with very few night shifts, and one-in-four weekends.
Candidates are expected to have a keen interest in gaining experience in Emergency Medicine at a Middle Grade level, with previous EM experience essential.
For further details on the post and how to apply contact ed.admin@hse.ie, or ramona.coen@hse.ie
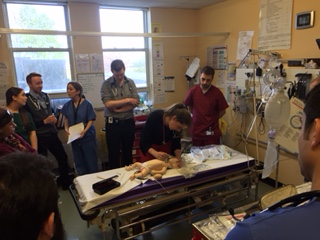
Busy morning today with our paediatric colleagues.
Simulated sick infant scenario in resus.
Well done to all who organized and took part.
PS Baby’s doing well
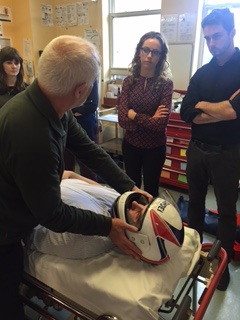


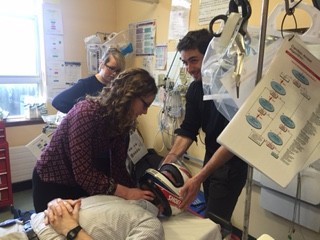
Medical Students attended an afternoon in training on sports-related pre-hospital emergencies.
Extraction techniques, spinal immobilisation and transfer, and airway management were covered.

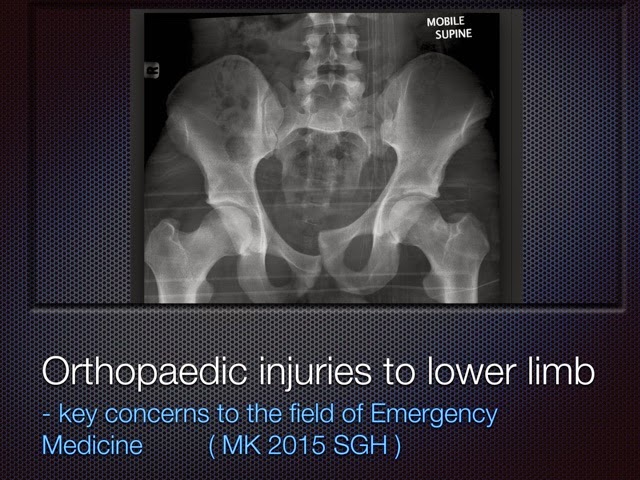
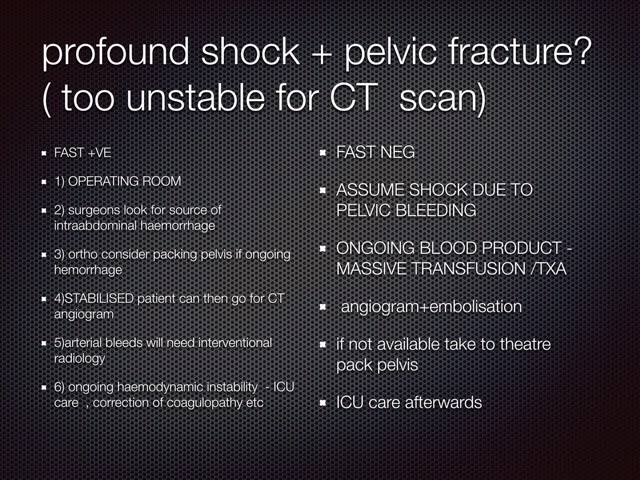
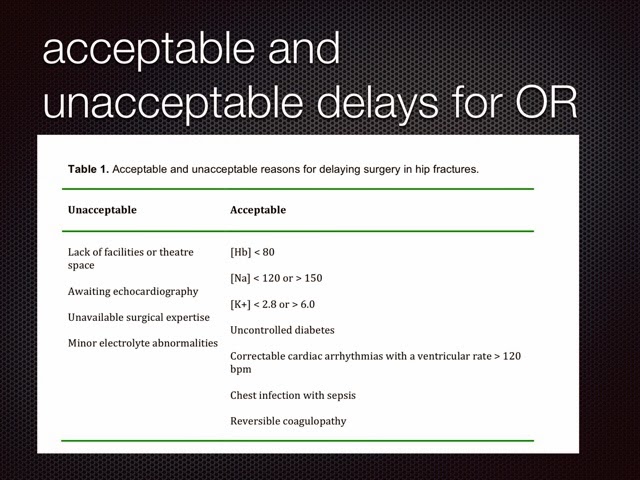
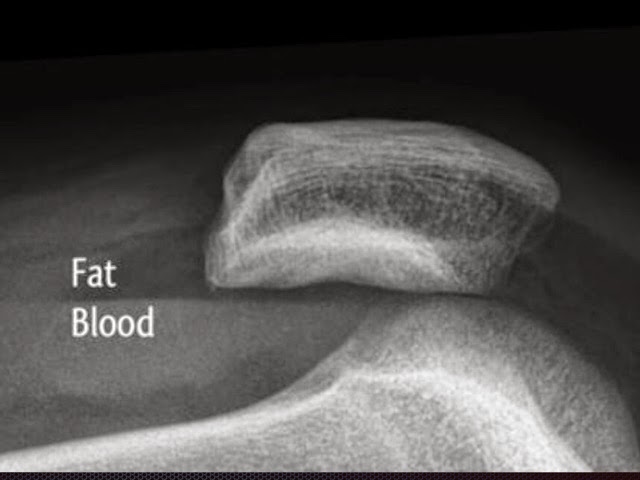
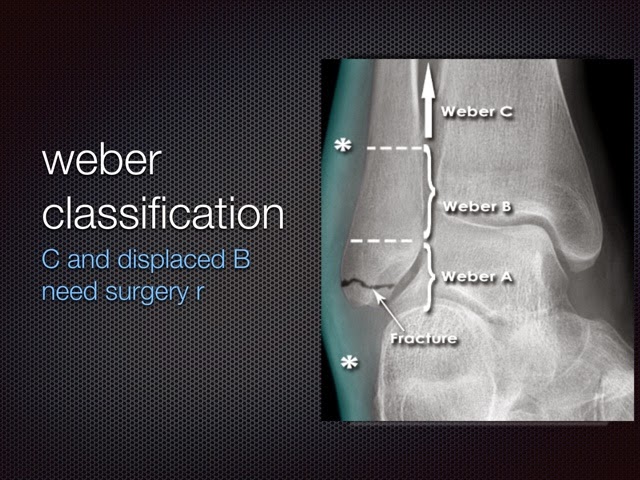
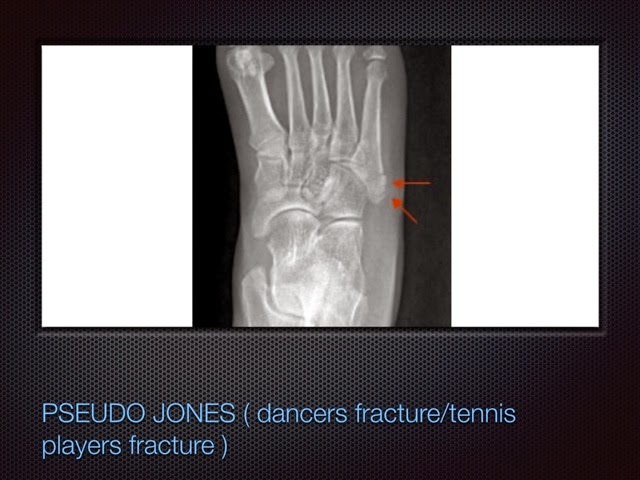
THE FOLLOWING IS A SUMMARY OF THIS THURSDAYS TALK ON LOWER LIMB INIJURY








Pre-Hospital Trauma Training Day for CSTEMS on 11th April in Ballina, Co. Mayo. Supervised by Consultants and SpRs in EM.
Any CSTEM trainees interested see attached flier
The Sligo Regional Hospital EM / Orthopaedics Rotation
NOTE:
THIS POST HAS BEEN FILLED FOR THE JULY 2015 INTAKE. If you are interested in applying for this post for January 2016 contact ed.admin@hse.ie
We have an exciting new vacancy available for SHOs from July 2015.
The successful candidate will spend 3 months as an SHO in Emergency Medicine and 3 months as an SHO in Trauma/ Orthopaedics.
If in the initial 6 months the performance is satisfactory, there may be opportunities for the candidate to complete a further 3 months in EM, and 3 months Acute Medicine.
This six/ twelve month rotation will offer the candidate a good introduction to Emergency Medicine in Ireland, and should put him/her in good position to apply for a formalized training program.
Candidates must be eligible for registration with the Medical Council of Ireland (http://www.medicalcouncil.ie/)
For further information on how to apply, please contact ed.admin@hse.ie
